|
Breastfeeding. We’ve done it since the dawn of time. And yet, before having a baby, we rarely stop to consider that it might be harder than it sounds! By the time we give birth we’ve heard from many well-meaning family members and health professionals that ‘breast is best’ and that ‘it is the biological norm’. So then, if we do encounter breastfeeding problems (like mastitis), it is easy to feel confused, guilty, overwhelmed or wonder ‘what is wrong with me?’  Please know that if you have/had mastitis you are not alone! In fact, mastitis affects up to 20% of breastfeeding women and occurs most commonly within the first six weeks after having a baby, but can occur at any time (Amir & Academy of Breastfeeding Medicine Protocol, 2014). Women who have had mastitis once are more likely to get it again, unless they receive the right help to correct the underlying causes. Unfortunately, women are often bombarded with conflicting information on how to best treat mastitis. And sadly, as a result women often feel that ceasing to breastfeed is the only realistic option they have. As a physiotherapist working in the field of women’s health on both a maternity ward and in a private practice, I treat many women with mastitis. It is a miserable, horrible and overwhelming time for new mothers. And it is so important that you get the right information as soon as possible. Here is some handy evidence-based info to get you started! What is Mastitis? Mastitis is inflammation of the breast (Amir & Academy of Breastfeeding Medicine Protocol, 2014). Milk ducts within the breast are designed for transporting breast milk, not for storing breast milk. Milk ducts are very easily squashed, so sometimes milk can cease to flow properly through the milk ducts due to factors like engorgement, blocked ducts etc. This results in milk products seeping from the milk ducts into the surrounding breast tissue. This causes a dramatic inflammatory response in the breast. Inflammation is essentially your immune system’s response to a stimulus that your body has flagged as a potential threat to your health and wellbeing. Your body sends all kinds of immune cells (think of these as ‘soldier cells’) to the affected area to help fight the other cells that your body thinks are the bad guys. In the case of mastitis, the foreign milk products escaping into the breast tissue are registered as foreign and a potential threat, so your body creates an inflammatory response to fight them. This is why you may feel sick, may have a fever, pain, breast swelling and redness. Taking over-the-counter anti-inflammatory medication (such as Voltaren or Neurofen) is generally safe whilst breastfeeding and can effectively help reduce the inflammation. If you are able to catch mastitis early enough, and manage the inflammation well, usually mastitis can be effectively treated without requiring antibiotics. That’s great news! (A note on infective mastitis: In some cases mastitis can be infective, but not in all. The only way of knowing whether it is infective or not, is if a milk culture is taken. As this is a time consuming process your doctor will normally decide whether or not to give you antibiotics based only on your clinical presentation. And whilst antibiotics will treat an underlying infection, they do not treat the inflammation associated with mastitis, nor do they correct the underlying factors that may have contributed to the development of mastitis. Therefore, it is important to address these other issues as well as taking antibiotics.)  Common symptoms of mastitis:
Common causes of mastitis:
Here are 5 important things you can do at the first sign of mastitis:
In summary, don’t suffer in silence! Pay attention to your breasts. Trust your intuition and listen to your body. If something doesn’t feel right seek help as soon as possible. There is plenty of help for mastitis and breastfeeding problems out there. By Christel Weston. Womankind Physiotherapy.  References
Amir, L. H., & Academy of Breastfeeding Medicine Protocol, C. (2014). ABM clinical protocol #4: Mastitis, revised March 2014. Breastfeed Med, 9(5), 239-243. doi:10.1089/bfm.2014.9984 Cooper, B. B., & Kowalsky, D. (2015). Physical Therapy Intervention for Treatment of Blocked Milk Ducts in Lactating Women. Journal of Womenʼs Health Physical Therapy, 39(3), 115-126. doi:10.1097/jwh.0000000000000037 Witt, A. M., Marinelli, K. A., Gill, S. L., Bolman, M., Kredit, S., & Vanic, A. (2015). Therapeutic Breast Massage in Lactation for the Management of Engorgement, Plugged Ducts, and Mastitis. Journal of Human Lactation, 32(1), 123-131. doi:10.1177/0890334415619439
3 Comments
 She came from my being. Started as a seed, always there. Never apart. Her number was chosen, she won and thrived; My bread was her bread, my lungs, her air. She was me. There was no divide. My rhythm was her lullaby. We became an alien, a two headed, strong willed force of nature. She came with a purpose, perfect from the start. She breathed her own oxygen and her blood pumped red. I didn’t think twice when they cut her physical bond to me. It didn’t even bleed a tear. We smiled. Why didn’t I mourn that more?  She did not recognise herself, rather knew herself only in relation to me. Without my body, my scent, my sounds; she was lost. My milk sustained and nourished her. She grew fat on it. She was physically, completely a product of my body. I was her world. It came with responsibilities; some of which were terrifically, physically, emotionally challenging. Others that were utter gluttony in their delight. And all she wanted was me, we were so wrapped in each other, We may as well have been one and the same. And we were.  She took food from a spoon and I mourned a little loss, Gone was the monopoly I had on her creation. She carried on the job of children; to grow and learn and become. Become a personality, an individual, an identity, a person. She found her voice, a beautiful husky utterance that I recognised as my own. We watched her stumble out her first steps and babble out her first words. Steps became skips and words became songs. She was blooming. And so was our love.  And all this time, she had been observing, Drinking in language, gestures, concepts. Lapping up information and gathering opinions. Lots of them mine, but then, a word I do not say, or a gesture that is foreign. There is a dart of panic. A loss of control. An extension of the cord Now she is at school. Now the tables have turned. I am here for food, for clothes, for transport, for sleep. But there are many hours and many teachers and many friends, shaping my baby. This walking, talking, running, jumping, skipping, thinking, writing, reading; baby of my body.  Then there are the moments before dawn, a little tip toe down the hall
There is a soft little voice and hand and she is curled in my body once again. Later, she will make her breakfast, dress herself, and run with friends But in this moment, rarer by the day, she has come home to rest. She is beautiful and she is mine. But when did she become apart from me? I will never know. And I will not hold her back. Though she may travel far and wide, She is my baby of my body, and always she will be. If you are suffering or have suffered with pelvic girdle pain (PGP) you know the painful ache that permeates one side of your lower back when your walking or getting dressed, or the sharp grabbing pain at the pubic bone, that pulls you up short when you take that first step from the couch. It can come and go, it can swap sides, it will ruin your sleep, and it can prevent you from being that active, happy pregnant lady you always thought you’d be. Read on to answer all your questions about PGP and how best to manage it. (Note: If it gets too heavy, you can skip to the summary cheat sheet at the end ;)) 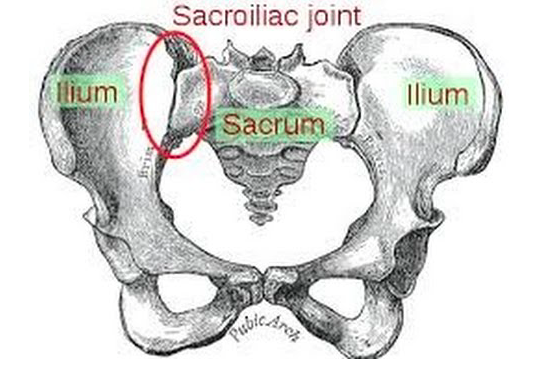 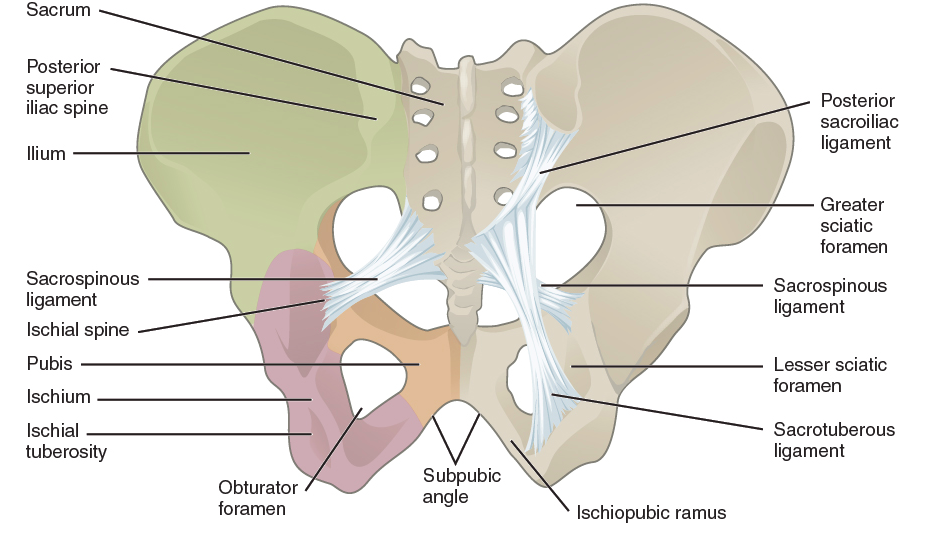 What? The pelvis is a bony ring made up of the sacrum and the ilia bones meeting at the cartilaginous pubic symphysis at the front of the body. The bony structure is reinforced by active and passive structures, (muscles and ligaments/fascia), that contribute to its stability. The role of the pelvis is to allow movement, and to transfer and absorb forces between the trunk and the limbs. In an upright position, the weight of the head, arms and trunk are transferred to the lower limbs through the sacrum, the sacro-iliac joints, the ilia bones, and into the femurs. For load to be smoothly transferred, movement at the sacroiliac joints must be minimised. The body does this in two ways: form closure and force closure. Form closure refers to the anatomical shape of the bones and the complimentary joint surfaces that cause the sacrum to form a keystone effect between the two ilia bones. During weight bearing the sacrum is forced downwards and tilts slightly forward (this is caused nutation). This causes a close-packed position of the sacroiliac joint and contributes to stability and efficient weight transfer. 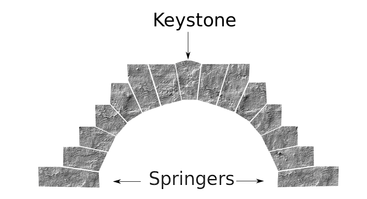 Force closure refers to ligaments, muscles and fascia that work across the joint to further compress and stabilise the bony surfaces. Nutation of the sacrum causes tightening of the sacroiliac ligaments. Muscles that cross the joint, (namely piriformis and gluteus maximus) will activate to provide additional stability. Additionally, studies have demonstrated that transverse abdominus, the inner-most abdominal muscle, contributes to stabilising the lower spine and the sacroiliac joints (Hodges, 1999). Where? PGP is described as pain experienced between the posterior iliac crest (top of the pelvis bone at the back) and the gluteal fold (the crease where your bottom finishes and your leg begins), predominantly at the level of the sacroiliac joints with or without referral into the back of the thigh. Pain can also be experienced in conjunction with, or exclusively in the pubic symphysis (the bone between your legs at the front).  When? PGP can occur at anytime, but most commonly presents during pregnancy or postpartum. During pregnancy, the expanding and increasing weight of the uterus puts a biomechanical strain on the body, in particular the lumbar spine and the pelvis. The load on local tissues causes creep (gradual stretch), which may contribute to stimulation of mechanoreceptors inducing increased activation of pain receptors. Creep also has implications for a change in proprioception (knowing where the body is in space), and therefore motor control, which means the brain’s ability to activate and control muscle sequences for optimal movement. Additionally, the growing abdomen during pregnancy leads to a change in the angle of pull of the deep abdominals, making them less effective for stabilising the sacroiliac joint. Pregnancy comes with an increase in the hormones; relaxin, oestrogen and progesterone, which contribute to increased soft tissue laxity. The contribution toward PGP each of these hormones makes is still unclear. A systematic review of the literature in 2012, looked at the relationship between relaxin levels and pelvic girdle pain in pregnancy. Three of the four high quality studies, found no association between relaxin levels and the presence of pelvic girdle pain. In other words, despite documented high levels of hormones and increased joint laxity, this does not always correlate with the presence of PGP. Who?  PGP is common during pregnancy, prevalence data from large studies show an agreed prevalence in a pregnant population of 20%. The recovery rate of PGP following pregnancy is high, with one study of 41,241 women reporting an 82.5% recovery rate in women who experienced pain during pregnancy. The overall prevalence of PGP experienced in the first three months postpartum is reported as 7%. The literature agrees that a more severe pain experience involving more than one pelvic joint during pregnancy is associated with an increased likelihood of PGP postpartum. Pregnancy and new parenthood is a time of great life-change, and brings stressors that are foreign and can seem insurmountable. Post-natal depression affects one in seven women and the ‘baby blues’ affects approximately 80% of new mothers. A lesser known condition is ante-natal depression which occurs during pregnancy and affects 10% of women (PANDA). Additionally, sleep deprivation to varying degrees impacts all new parents. Sleep deprivation has been found to cause hyperalgesic changes in the body, which contribute to chronic pain. PGP must be approached within a biopsychosocial framework. Pain is influenced by cognitive and psychosocial factors that modulate pain amplification and disability levels. It is known that ongoing pain can be centrally mediated by the forebrain, it is therefore understandable that PGP disorders can potentially be induced and /or maintained through a balance of peripheral physiological mal-adaptive behaviours, and centrally mediated pain sensitisation. Why? Putting all the who, what, where, and when together brings us to the why? So, we know the sacroiliac joint requires stability to function, that is, to transfer weight efficiently and pain-free from one leg to another. Factors that reduce this in pregnancy are increased ligament laxity, decreased efficiency of muscle activation through altered proprioception and motor control, and in the case of abdominals, less efficient angle of pull. Combine this with an increased load to transfer as the uterus expands with the growing foetus and the pelvis has it’s work cut out. However, still only one in five women will experience pelvic girdle pain. So, why? Well joint stability is not about how resistant structures are to movement or how much movement is available but instead, about the motion control that allows load to be transferred and movement to be smooth, effortless and painfree (Vleeming et al., 2008). Meaning, that it is the complex interplay between these factors that combine to present as pain. How is PGP managed? Physiotherapists have many tools that we use to reduce pelvic girdle pain, these include: -External Pelvic Compression with Belts/Tape/Compression garments -Soft Tissue Mobilisation -Hot/Cold Therapy -Activity Modification/Education -A Specific and Individualised Exercise Program.  Accurate movement analysis and postural assessment is essential to long term recovery. Many studies have analysed exercise regimes; common theories are Vleeming’s anterior/oblique, posterior and vertical muscular slings. Or the functional activation pattern initially proposed by Stuge and her team in 2004 which begins with strengthening local stabilising muscles such as transverse abdominus, pelvic floor and multifidus prior to building in more global stabilisers such as latissimus dorsi, gluteus maximus, abdominal obliques and hip adductors and abductors. Results vary between studies, but there is a trend in the literature to support individualised, exercise prescription that emphasises deep stabilising muscle activation, and functional progression received one-to-one by physiotherapists over at least 6 weeks. It can be concluded that global muscles alone, despite ability to increase stability of the SIJ, have no impact and may potentially exacerbate symptoms if not recruited in an activation pattern that includes local core stabilisers of the lumbo-pelvic region as well. Supervision of exercises is important to ensure quality of exercise performance and to translate to pain reduction. Summary (the cheat sheet):  Whether you have symptoms of PGP, have had symptoms, or are a health practitioner who see’s patients with PGP, I hope you got something out of this information that will help you. I practice women’s health physio in Lower Plenty, Melbourne and regularly care for women with acute and chronic PGP. I am always happy to chat and share information, so feel free to make contact with me at any time. Kym References: Albert H, Godskesen M, Westergaard J (2001) Prognosis in four syndromes of pregnancy-related pelvic pain. Acta Obstet Gynecol Scand 80:505–510 Heckman JD & Sassard R (1994) Musculoskeletal considerations in pregnancy. Journal of Bone and Joint Surgery American Volume 76, 1720–1730. Hodges PW (1999) Is there a role for transversus abdominis in lumbo-pelvic stability? Manual Therapy 4, 74–86. Lautenbacher, S., Kundermann, B., Krieg, J. (2006). Sleep deprivation and pain perception. Sleep Medicine Reviews. 10(5): 357-369. Lillios, S., Young, J. (2012). The Effects of Core and Lower Extremity Strengtheinin on Pregnancy-Related Low Back and Pelvic Girdle Pain: A Systematic Review. Journal of Women’s Health Physical Therapy. 36(3): 116-124. Marnach, M., Ramin, K., Ramsey, P., Song, S., Stensland, J., An, K. (2003). Characterization of the relationship between joint laxity and maternal hormones in pregnancy. Obstetrics and Gynecology. 101(2): 331-335. Ostgaard, H., Zetherstrom, G., Roos-Hansson, E., Svanberg, B. (1994b). Reduction of back and posterior pelvic pain in pregnancy. Spine. 21:2777-2780. Pennick, V., Liddle, S. (2013). Interventions for preventing and treating pelvic and back pain in pregnancy. Cochrane Database of Systematic Reviews. 8. Schauberger, C., Rooney, B., Goldsmith, L., Shenton, D., Silva, P., Schaper, A. (1996). Peripheral joint laxity increases in pregnancy but does not correlate with serum relaxin levels. American Journal of Obstetrics and Gynecology. 174: 667-71. Stuge, B., Veered, MB., Laerum, E. et al. (2004). The efficacy of a treatment program focusing on specific stabilising exercises for pelvic girdle pain after pregnancy: a two-year follow up of a randomised clinical trial. Spine. 29:197-203. Vleeming, A., Stoeckart, R., Volkers, A., Snijders, C. (1990). Relation between form and function in the sacroiliac joint. Part 1. Clinial anatomical aspects. Spine. 15: 130-132. Vleeming, A., Volkers, A., Snijders, C., Stoeckart, C. (1990b). Relation between form and function in the sacroiliac joint. Part 2. Biomechanical aspects. Spine. 15:133-136. Vleeming et al. (2008). European Guidelines for the diagnosis and treatment of pelvic girdle pain. Spine. 17:794-819. Vermani, E., Mittal, R., Weeks, A. (2010). Pelvic Girdle Pain and Low Back Pain in Pregnancy: A Review. Pain Practice. 10(1): 60-71.  Pregnancy, Labour, Breastfeeding, Parenting. Lots of people have done it, lots of people are doing it. Lots of people want to tell you how to do it. As a new mum, or back up, as soon as you announce your pregnancy, people are full of stories and anecdotes about their experience, and very keen to pass on well intended ‘words of wisdom’. And unfortunately, you also get conflicting messages and advice from the bevy of health professionals you come in contact with, particularly in those early, sleep deprived days as you are beginning your life as a parent. Breastfeeding issues? Oh you need to express more. No! Baby to breast ALL the time. More sleep will do the trick! Rub breast milk over your nipples after every feed. No! Get the lansinoh on it! Just some fresh air and sunshine is all you need! Massage the lump toward the nipple, NO - away! Heat before a feed and cold after. More time between feeds, feed as often as you can to keep the milk moving! AAAAAHHHHHHHHGGGG!!!!! It makes me stressed even writing it. I’m going to say something now that could well put me out of a job. You already know what to do. The reason you think you don’t is not your fault. It’s a combination of access to too much information and bad old wives tales. Let me paint you a picture. I see women who have blocked ducts or mastitis. These are the sickest women in my care. They come in and when they’re in the thick of it, they are clammy, spaced out and desperate. Not only are they very sick, but they are sleep deprived (cos they’re a mum of a newborn), in a state of physical recovery (cos they’ve just given birth), and they are stressed to the max because their baby’s lifeline (their breast) is under very serious threat. You know what makes mastitis worse? Stress. You know what stresses a mum more than anything? Feeling confused and helpless. Now, there is lots I can do for this lady but the best thing I can do right away is tell her to TRUST HERSELF. You’re a mum now, that comes with instincts. Trust them, they’re good. More than anyone’s advice, more than the doctor, more than the midwife, the lactation consultant and more than my advice, do what feels right for you and your baby. The feeling I get when I see the lady’s reaction is bitter sweet. I love that look of relief, enlightenment and trust; but I hate that the reason they understand what I’m saying is because they have been made to think they don’t know what’s best. Not by any one person in particular, in fact, the most reliable culprit will be themselves, that good old self doubt we are all so good at. An injection of self belief and an excuse to stop wasting precious time googling their condition for a better answer can work miracles. To all mum’s out there, you already know what to do. Stop and listen to your baby and your body, and trust yourself. Then get some rest. That’s always my second piece of advice :)   A lot of people, mostly clients, ask me why I got into pelvic floor physiotherapy. Often the question comes just as I'm about to do an examination and often it's framed like; “How did a nice, young girl like you find yourself doing something like this?” I normally respond by saying "Well, having a couple of kids makes you interested in the pelvic floor!" or "I think it's the area in physio where I can have the greatest effect on people's quality of life". Both of these statements are very true. But the real reason I became interested and specialised in women's health is that after my first baby, Lily who is now aged 7. I developed a vaginal prolapse. I was 24, and felt like I was falling apart. I was so horrified that someone like me, a physio with information and education on how to look after my body during pregnancy and postpartum, had still developed a prolapse. I felt defeated. It sent me into a spiral of depression and self pity about my physical future and the possibility of having more children. How had no-one warned me about this? Where had I gone wrong? Was I expected to live with this diagnosis and sensation for the rest of my life? I started learning everything I could about prolapse and pelvic floor health. One thing led to another and I was sitting in a post-graduate class at Melbourne Uni studying Advanced Rehabilitation of the Pelvic Floor, I loved it, so enrolled in another course this time, studying Exercise for Women. I realised there was so much more we needed to do to get the right information out there to pregnant and postpartum women. So, where had I gone wrong? Despite the fact I should have known better, I had let my pride get the better of me. I had conformed to what I saw on magazine covers and Facebook feeds and tried to return to my pre-pregnant self within weeks of delivering my baby. It wasn’t necessarily about looking great, it was just about being independent and capable. I picked up prams, grocery bags, washing baskets, even assisted packing and lifting boxes when we moved house at 6 weeks post partum. I was determined to be seen by everyone, as one of those women, who are competent, successful and fabulous. It's not to say the information about how to do it better wasn't out there. It's just that the noise from my newsfeed of stories about women 'bouncing back' was so much louder and frankly, more exciting. But even if I may have fooled a few friends or family as to my competency or fabulousness, it was skin deep, and not worth it. So, I now spend a lot of time discussing these issues with my family, friends and very importantly the women in my professional care. It is a driving passion for me to educated women about how pregnancy, labour, birth and postpartum recovery not just should be done, but HAS to be done. It is my goal to dispel myths and images of perfection like this… And saturate my community with real images like this…. I am very pleased to say that now, I am no longer bothered by symptoms of my prolapse. I delivered my second baby, Eliza (who was 4.6kgs), 3 years after Lily was born. I heeded all my own information about optimal recovery immediately postpartum and long term, and my prolapse stayed at bay. I now regularly participate in fun runs, lift weights at the gym and jump on the trampoline with my kids. Prolapse management and pelvic floor health will always be on the agenda for me, as it should be for everyone. But hopefully, my story and my message will mean less young women are diagnosed due to impossible and unrealistic pressures they may be putting on themselves.
|
Welcome!Hi! Welcome to The Blog! Please be aware, Womankind Physiotherapy's blog is not intended to replace information and advice from your health care provider. For specific concerns regarding your health you must seek individualised care by your preferred provider.
Archives
March 2021
Categories
All
|




 RSS Feed
RSS Feed